
Vitamin D3 (cholecalciferol) stands out among the most common forms of vitamin D in the human diet. Vitamin D3 is mostly found in animal-sourced foods, such as eggs (especially yolks), cheese (in particular, cheddar), fatty fish (such as sardines or salmon), and yoghurt. Meanwhile, the most common problems of vitamin D3 deficiency include depression, developing osteoporosis, difficulties in walking, fatigue and malaise feeling, and muscle aches.
Vitamin D plays a paramount role in regulating bone growth and promoting the absorption of calcium. In essence, the human skin produces vitamin D during exposure to sunlight. However, when people live at high latitudes or spend most of their time indoors, they need to get vitamin D from their diet. With that in mind, fish oils, fatty fish, egg yolk, butter, and liver remain the best dietary sources of vitamin D. At the same time, one might face difficulties in getting adequate amounts of the nutrient from diet alone. Therefore, billions of people across the world experience vitamin D deficiency and consume supplements.
Comes with 30 day money back guarantee
Shop now
Whenever you regularly lightly clad without sunscreen or spend sufficient time outdoors, you may be getting all the vitamin D you need. However, in countries farther away from the equator, this duration of exposure does not apply, and you might need more time to achieve similar results. Still, one should keep in mind that sunburns remain a major risk factor for skin cancer. Hence, you should be careful and avoid spending too much time in the sun without sunscreen, especially with light-coloured skin.
Vitamin D represents a family of vitamins with a similar chemical structure. The most commonly found members of vitamin D in the human diet include vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). Those types differ in a few important ways, though both of them help people meet their vitamin D requirements.
In this article, we will explore the health benefits of vitamin D3 and the differences between vitamin D2 and vitamin D3.
Vitamin D2 and Vitamin D3: What Is the Difference?
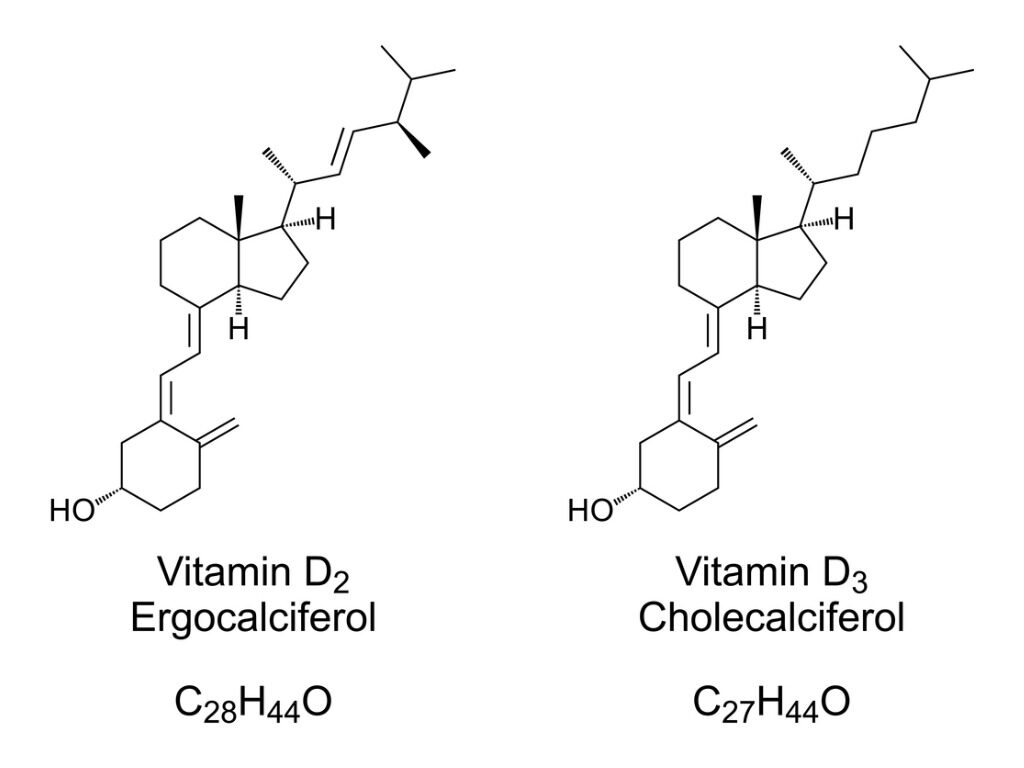
Vitamin D2 and vitamin D3 differ according to their food sources. In particular, Vitamin D3 is only found in animal-sourced foods, while D2 mostly comes from fortified foods and plants. Since, vitamin D2 is cheaper to produce than vitamin D3, this makes it the most common choice for fortified foods. As for vitamin D3, the skin produces it during sunlight exposure. In particular, ultraviolet B (UVB) radiation from sunlight invokes the formation of vitamin D3 from the compound 7-dehydrocholesterol located in the skin. A similar process takes place in mushrooms and plants, where UVB light triggers the formation of vitamin D2 from ergosterol, a compound from plant oils.
When it comes to upgrading your vitamin D status, vitamin D2 and D3 are not equal despite both being effectively absorbed into the bloodstream. The liver metabolizes vitamin D2 and vitamin D3 into 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3 accordingly, collectively known as calcifediol or 25D. This is the vitamin D complex, which circulates in the blood and directly reflects the levels of vitamin D in the body’s stores. Calcifediol is also commonly cited as the “active form” of vitamin D. Health professionals usually measure calcifediol (25D) levels when they order lab tests to check vitamin D amount in the body.
Most studies confirm that vitamin D3 remains more efficient at raising blood levels of calcifediol than vitamin D2. For instance, one study in 32 older women has established that a single dose of vitamin D3 was twice more effective compared to vitamin D2 at raising calcifediol levels. Some scientists have even raised concerns about whether vitamin D2 supplements could be of lower quality than D3 supplements due to being more sensitive to fluctuations in temperature and humidity. For these reasons, vitamin D2 supplements could degrade quickly over time. Nevertheless, it is pretty unknown whether this information is relevant to human health.

Several studies have also researched whether supplementation with vitamin D2 or D3 produced a higher blood level of calcifediol. One studyissued by the National Institutes of Health has explored post-menopausal elderly women with vitamin D deficiency. The study compared the effects of receiving a single high dose of vitamin D2 or vitamin D3 on calcifediol levels. Eventually, vitamin D3 produced about twice the amount of circulating calcifediol in the selected population group versus that of vitamin D2.
A separate clinical trialcompared a ten-week regimen of twice-weekly 50,000 IU dosing of both vitamin D2 and vitamin D3 in demographically matched groups. As a result, vitamin D3 has also been found to show a superior effect in producing higher levels of or calcifediol compared to vitamin D2.
Still, consumers should not worry about the quality of their vitamin D2 supplements until new research proves otherwise. Some storage measures should be met, though, such as keeping the supplements at room temperature, in a closed container, out of direct sunlight, and in a dry place.
Vitamin D2 and Vitamin D3: When Should We Take?
Cholecalciferol (also known as vitamin D3) is applied as a dietary supplement in case of the lack of vitamin D in the diet and remains within a class of medications called “vitamin D analogs”. The body requires cholecalciferol for healthy bones, muscles, nerves and to support the immune system. Vitamin D3 helps the body to employ more of the calcium located in foods or supplements.
People facing vitamin D deficiency typically include breastfed infants, people with dark skin and limited sun exposure, older adults, obese people, patients suffering from a gastrointestinal disease (GI), Crohn’s disease, and celiac disease. Cholecalciferol is also used alongside calcium to prevent and treat bone diseases such as osteomalacia (softening and weakening of bones resulting from vitamin D deficiency), osteoporosis (a condition when the bones get thin and weak and break easily), and rickets (softening and weakening of bones in children caused by lack of vitamin D).
Cholecalciferol typically comes as a gel capsule, capsule, chewable gel (a.k.a. gummy), liquid drops, or a tablet. People usually take it once or twice daily depending on their age and medical condition. Cholecalciferol supplements often come in combination with other medications and vitamins. Cholecalciferol is usually sold without a prescription. However, doctors might prescribe it to treat certain conditions. Cholecalciferol liquid drops can be added to children’s food or drink.
All forms of vitamin D3 supplements are available over-the-counter (OTC). Hence the FDA does not allow the production companies to make treatment claims. Still, vitamin D3 is frequently used off-label to treat vitamin D deficiency, hypoparathyroidism and prevent osteoporosis.
As for vitamin D2, it is often prescribed to treat hypoparathyroidism (decreased thyroid hormone secretion), vitamin D resistant rickets, and hypophosphatemia (low levels of phosphorus in the blood). Vitamin D2 is commonly used in both over-the-counter formulations for vitamin D insufficiency and prescription. However, the FDA does not support treatment claims for over-the-counter vitamin D2 supplements.
Regarding the drug interactions of vitamins D2 and D3 with other medications, they are quite possible. When taken with aluminum hydroxide, Vitamin D might precariously increase the serum levels of aluminum. Hence, this combination should be avoided. Hydrochlorothiazide, among other types of thiazide diuretics, might increase calcium levels in the blood to a dangerously high level when combined with vitamin D. Therefore, health professionals should monitor the people prescribed with both thiazide diuretics and vitamin D supplementation. Certain drugs might also reduce the absorption rates and effectiveness of vitamin D supplements. Cholestyramine, and other bile-acid sequestrants, are the example of drugs that will impede vitamin D absorption. Hence, cholestyramine should not be administered with vitamin D at the same time.
The Health Benefits of Vitamin D3
Vitamin D3 has a direct role in many aspects of health and also might have an impact on up to 2,000 different genes within the body. Vitamin D receptors are located in almost every cell. When vitamin D3 binds to a cell receptor, it turns some genes on or off, thus inducing changes at the cellular level. Certain studies have suggested that binding vitamin D3 might turn on immunoprotective genes, turn off cancer-causing genes, and even command cells which minerals to absorb.
In addition, vitamin D3 influences many other important body processes, such as:
Healthy bones often result from good vitamin D3 admission since it helps to control and regulate the body’s ability to soak up calcium and phosphorus. These two compounds provide strength and density to the skeleton and teeth.
The presence of vitamin D can also impact heart function. Several studies have shown that insufficient levels of vitamin D might correlate to an increased probability of a heart attack. Some researchers also believe that vitamin D might keep heart muscle cells from growing too large and improve cardiovascular endurance. Consequently, this prevents the thickening of the walls of the ventricles, which might cause a heart attack by blocking blood flow.
Vitamin D3 braces the pancreas and sets off the process of insulin production. This is essential for efficient management of blood sugar levels and helping diabetics to have better control over the disease.
According to the study from Boston University, people with high blood pressure used to experience relief after the increase of vitamin D3 levels. This is because vitamin D3 significantly reduces renin concentration. Renin stands for an enzyme produced by the kidney with an effect on blood vessels.
Positive impact on mood stands among the most significant benefits of vitamin D3. Many people generally feel a way happier when the sun shines after suffering from the seasonal affective disorder. This is because the synthesis of vitamin D3 happens during direct exposure to UVB rays. Also, the increase of vitamin D consumption could effectively reduce the symptoms of clinical depression alongside other treatments.
Some research suggests that by increasing vitamin D3 consumption, it is possible to slow the progress of prostate tumors. Other studies show promise that combining vitamin D3 with more fiber might reduce the risk of developing polyps leading to colon cancer.
The combination of vitamin D3 and calcium remains another helpful combination. A four-year trial established that those post-menopausal women who received both vitamin D3 and calcium supplements had a 60% less likelihood of developing cancer. Scientists have also studied Vitamin D3 for the potential treatment of breast cancer. In the study of 166 women under treatment, approximately 70% had lower levels of vitamin D.
Vitamin D3 Deficiency and Its Consequences
In recent years, doctors have started to treat vitamin D deficiency and its consequences more seriously.
The most common problems of vitamin D deficiency include:
- Depression
- Developing osteoporosis
- Difficult walking
- Fatigue and malaise feeling
- Muscle aches and weakness
- Pain in bones leading to stress fractures
According to some estimations, approximately 32% of adults and children are deficient in vitamin D3, and about 50% of the world population remains at risk for developing a vitamin D3 deficiency, mostly due to the sun factors.
They include:
- Darker skin tone that is capable of absorbing a smaller amount of sunlight
- Living in highly polluted areas, which filter out UV rays
- Living in areas with little direct sunlight, especially in areas with tall buildings
- Spending more time indoors than out
- Taking certain medications that might reduce vitamin D3 levels, for example, barbiturates and statins
- Working ‘graveyard’ shifts without an opportunity to get into the sun regularly
In order to prevent vitamin D3 deficiency, one might take several measures. Apart from getting more sun, people might find the nutrient in a range of foods such as eggs, cheese, sardines, salmon, and yoghurt.
Supplemental vitamins might also help, especially the recommended intake of 1,000 IU per day. At the same time, receiving clearance from a health professional remains crucial. A blood test is usually sufficient to determine vitamin D3 deficiency and daily dosage.
Vitamin D3 and Contemporary Diseases
- Neurodegenerative disorders
Today, vitamin D3 deficiency has been implicated as serving a role in a number of neurodegenerative disorders, despite the lack of sufficient clinical research. At the same time, there is rather entrancing evidence that low levels of vitamin D3 create an additional risk factor for multiple sclerosis (MS). MS is a dangerous condition when the immune system attacks the central nervous system and causes axon degeneration and demyelination. In many instances, MS is related to decreasing exposure to solar UV radiation. Some studies suggest that a lower risk of MS corresponds to high circulating levels of vitamin D3.
There is also certain evidence that vitamin D3 deficiency is relevant to Alzheimer’s disease and Parkinson’s disease. In particular, treating ageing rats with calcitriol prevented decreases in neuron density and reduced hippocampus shrinkage. These results imply that vitamin D3 could have a preventive role in treating neurodegenerative disorders, although more research into this area is needed.

- Vitamin D3 and COVID-19 Pandemic
Vitamin D has split scientists during the COVID-19 pandemic. While several studies have claimed that vitamin D and its forms can fight coronavirus, others argued that it was of no benefit. Nevertheless, the recent UK Government review has confirmed that there was a lack of sufficient evidence that the increase in the daily dosage of vitamin D or D3 could prevent or somehow treat COVID-19. A number of experts from multiple Government agencies, including Public Health England, examined different scientific studies from around the world. Subsequently, the selected team, introduced by the National Institute for Health and Care Excellence (NICE), made the conclusion that a direct relationship between COVID-19 and the deficiency of vitamin D and its forms was ‘not possible’ due to insufficient trials.
At the same time, certain studies have confirmed that many people getting COVID-19 do not have sufficient levels of vitamin D in their bodies. Moreover, the sickest patients are often deficient in vitamin D and D3. Still, the question remains whether getting infected causes vitamin D levels to rapidly fall down or whether the deficiency of vitamin D makes people more vulnerable to COVID-19. Therefore, NICE urges the UK population to take no less than ten mg (400 IU) of vitamin D or its forms daily from October till early March.
Arguments on the link between poor COVID-19 outcomes and vitamin D deficiency started to emerge as early as May 2019. However, the lack of gold-standard medical research remains the major problem. Only the University of Cordoba in Spain has conducted some serious research up to date. In particular, the researchers distributed high doses of calcifediol, also known as vitamin D3, to 50 patients diagnosed with COVID-19. There were zero registered deaths among the volunteers who received the vitamin. Nevertheless, however, two of the 26 patients in a control group without calcifediol died. Only one patient who took calcifediol was brought to intensive care, while half of the participants in the control group went to ICU.
Still, several scientists have denounced the study on the basis of small sample size, insignificant to make firm conclusions regarding the impact of vitamin D3 on COVID-19 patients. However, the study by the University of Cordoba remains the most promising on the subject up to date and corresponds to earlier research that eliminating vitamin D3 deficiency might cut mortality rates from COVID-19 pandemics.
The studies by Tehran University and Boston University have shown that hospitalised patients with COVID-19 with sufficient vitamin D levels were 51.5% less likely to die from the virus. The later analysis of 235 hospitalized patients with COVID-19 also suggested that patients with sufficient vitamin Dlevels had a particularly lower risk of falling seriously ill and requiring ventilation. Moreover, patients with an abundance of vitamin D experienced less inflammation. However, this study has also had certain weaknesses, such as taking into account such corresponding factors as smoking and social-economic status.
Currently, researchers from the Queen Mary University of London perform a randomized trial on the possible beneficial impact of taking vitamin D and its forms on patients with COVID-19. In October 2020, a group of 5,000 volunteers was tasked with receiving high vitamin D doses for regular consumption during the following six months. Experts will then assess whether the participants were at lesser risk of getting COVID-19 and developing a severe state of the disease during the winter.

- Vitamin D3 and Pre-Menopausal Women
Supplementation with a combination of vitamin D3 and omega-3 may have multiple health benefits on pre-menopausal women with vitamin D deficiency, say Jordanian researchers. Some studies also report a relationship between estrogen metabolism and vitamin D. The decline of estrogens during menopause results in a decrease in bone density, increased bone turnover, and elevated fracture risk. Musculoskeletal discomfort might facilitate mood disturbances, impair quality of life, and increase the risk of cardiovascular disease. Vitamin D deficiency might aggravate multiple diseases that occur during menopause. Taking into account that menopause and vitamin D deficiency generate risk factors beyond bone health such as affective, cardiovascular, cognitive, and metabolic disorders, all peri- and post-menopausal women should strive to obtain sufficient vitamin D status.
Older women, especially those who are not exposed to sunlight for staying homebound, remain at risk of vitamin D3 deficiency. Hence, women aged 19 to 50 ideally should take 15 mg (600 IU) of vitamin D on a daily basis. Women over 50 should receive a higher dose, up to 20 mg (800 IU). Even though it is possible to follow a diet rich in vitamin D, the best solution is still to take a supplement.
People should abstain from consuming cholecalciferol in the following circumstances:
- Allergic reaction to vitamin D
- Hypercalcemia (high levels of calcium in the blood)
- Hypervitaminosis (high levels of vitamin D in the body)
- Malabsorption (any condition that makes it difficult for the body to absorb nutrients from food)
Additionally, people should inform healthcare professionals if they have ever had allergies, diabetes, electrolyte imbalance, kidney disease, or heart disease. Pregnant and breastfeeding women should also consult doctors on the use of cholecalciferol since too much vitamin D3 can potentially harm a nursing baby or an unborn baby. Parents are advised to abstain from giving cholecalciferol to children without medical advice.
Generally, no common side effects have been observed in therapy involving either vitamin D2 or D3. In most cases, side effects related to vitamin D result from hypervitaminosis D, a very rare condition that occurs in case of overconsumption of vitamin D. This is sometimes seen in patients who take megadoses of vitamin D, leading to vitamin D toxicity. Thus they build up dangerously high levels of calcium in the blood leading to constipation, frequent urination, nausea, and vomiting. When left untreated, calcification of organs and soft tissues can occur alongside irreversible renal failure.

Vitamin D regulates bone growth, plays a crucial role in immune function, and promotes the absorption of calcium. The human skin produces vitamin D during exposure to sunlight. However, when people spend most of their time indoors or live at high latitudes, they need to get vitamin D from their diet. Butter, egg yolk, fish oils, fatty fish, and liver remain the best dietary sources of vitamin D.
The most common forms of vitamin D in the human diet include vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). These two forms differ from each other according to their food sources. In particular, D2 mostly comes from fortified foods and plant sources, such as mushrooms, while vitamin D3 is only found in animal-sourced foods. Vitamin D2 is cheaper in production than vitamin D3. Hence it remains the most common choice for fortified foods.
Most existing studies suggest that vitamin D3 remains more efficient at raising blood levels of calcifediol than vitamin D2. Some scientists have even raised questions about whether vitamin D2 supplements were of lower quality than D3 supplements due to being more sensitive to fluctuations in humidity and temperature. Nevertheless, it is pretty unknown up to date.
Despite the lack of sufficient clinical research, vitamin D3 deficiency has been considered as one of the leading factors in a range of neurodegenerative disorders. At the same time, there is sufficient evidence that low levels of vitamin D3 contribute to an additional risk factor for multiple sclerosis. There is also certain evidence that vitamin D3 deficiency relates to Parkinson’s disease and Alzheimer’s disease.
People should abstain from consuming cholecalciferol due to the following conditions: hypercalcemia (high levels of calcium in the blood), hypervitaminosis (high levels of vitamin D in the body), malabsorption (any condition that makes it difficult for the body to absorb nutrients from food), as well as an allergic reaction to vitamin D.
All kinds of vitamin D3 supplements are usually available over-the-counter. Hence the FDA prevents the production companies from making treatment claims. Still, vitamin D3 is frequently used off-label to treat hypoparathyroidism, vitamin D deficiency, and osteoporosis.
Generally, no common side effects have been observed with the use of vitamin D2 and D3 in therapy. In most instances, vitamin D-related side effects result from hypervitaminosis D, a very rare condition that might happen after the overconsumption of vitamin D. This is sometimes seen in patients who take large doses of vitamin D and later experience vitamin D toxicity.

Anastasiia Myronenko
Anastasiia Myronenko is a Medical Physicist actively practicing in one of the leading cancer centers in Kyiv, Ukraine. She received her master’s degree in Medical Physics at Karazin Kharkiv National University and completed Biological Physics internship at GSI Helmholtz Centre for Heavy Ion Research, Germany. Anastasiia Myronenko specializes in radiation therapy and is a fellow of Ukrainian Association of Medical Physicists.