
Alzheimer’s disease (AD) is a neurocognitive disorder, which significantly impacts everyday life. As being the most common cause of dementia, AD contributes to substantial memory loss, impairment of language, problem-solving, and other thinking abilities.
According to statistics, AD is a real cause of up to 60 to 80% of the elderly people population, obviously varying in the mildness of disease. According to estimates, in the United States, 10% of people older than 65 have Alzheimer’s ailments.
It is predicted that over 120 million people will have AD by 2050 due to a lengthened lifespan. Percentage of people with progressive symptoms increase with age:
- From the age of 65 to 74: 3%
- From the age of 75 to 84: 17%
- From the age of 85 and older: 32%
Chances of dementia increases as brain inflammatory processes are often ongoing, and they build up as we age. Additionally, such an increase can be triggered by various factors like head injuries, alcohol abuse, or other disease processes.
AD is more common in women. Such a suggestion is possibly associated with a higher level of women’s life expectancy. The predominance of patient numbers in developed countries is related to the increase in the number of older people.
AD Clinical signs
Patients have symptoms and signs of dementia, which affects all aspects of life, but it takes time for dementia to develop. The most common first manifestations of AD are:
- Loss of short-term memory (for example, people who ask repetitive questions, often misplace items, or forget their purpose).
Other cognitive disorders tend to involve many functions, including the following:
- Impaired reasoning and problem solving, poor judgment (for example, patients may not be able to manage a bank account, make poor financial decisions).
- Linguistic dysfunction (e.g., difficulty thinking with ordinary words, speech and/or writing errors).
- Dysfunction of visual-spatial orientation (e.g., inability to recognize faces or everyday objects).
- Alzheimer’s disease is a progressive disorder, but may also have periods of stable, non-progressive course (plateau).
- Behavioral disorders (e.g., vagrancy, agitation, loudness, persecutory delusions) are also common.
Mechanism of formation
Mutations in genes encoding the synthesis of amyloid precursor proteins (presenilin I and presenilin II) can lead to autosomal dominant forms of Alzheimer’s disease even before old age. Thus, in sick individuals, the synthesis of amyloid precursor proteins is impaired, which leads to the accumulation and deposition of fibrillar aggregates of beta-amyloid, in turn, beta-amyloid is the main component of senile plaques, which consist of degeneratively altered axons or dendrites, astrocytes and glial cells located around the amyloid nucleus.
Two hallmarks of Alzheimer’s disease are:
- Extracellular beta-amyloid deposits (in senile plaques);
- Intracellular neurofibrillary tangles (paired coiled filaments).
Beta-amyloid deposition and neurofibrillary tangles result in the loss of synapses and neurons, which in turn leads to gross atrophy of the affected areas of the brain, typically beginning in the medial temporal lobe.
The mechanism by which amyloid-beta peptide and neurofibrillary tangles cause this damage is not fully understood. There are several theories.
The amyloid hypothesis states that progressive accumulation of amyloid-beta in the brain causes a complex cascade of events resulting in neuronal death, loss of neuronal synapses, and progressive neurotransmitter deficiencies; all of the above contributes to the development of clinical symptoms of dementia. Researchers agreed that one possible explanation for such abnormal protein accumulation is the variety of genetic mutations in these proteins.
Prion mechanisms have been identified in Alzheimer’s disease. In prion diseases, a healthy cell surface protein called prion protein is converted to a pathogenic form called a prion. The prion then triggers the conversion of other prion proteins similarly (like a virus), resulting in a marked increase in abnormal proteins, resulting in brain damage. It is believed that in Alzheimer’s disease, beta-amyloid in cerebral amyloid deposits and tau in neurofibrillary tangles are of the prion type with the property of self-reproduction.

The etiology of AD is multifactorial. Between 5 and 15% of cases are familial, half of which are early-onset (younger than 65 years of age) and are usually associated with specific genetic mutations. At least five different loci, located on chromosomes 1, 12, 14, 19, and 21, influence the onset and progression of Alzheimer’s disease.
The most common mutations occur in several proteins: APP, PS1, PS2, and the most common gene APOE-4. The last one is the first risk gene identified and remains the gene with the most substantial impact on being at risk. Researchers estimated that between 40-65% of people diagnosed with Alzheimer’s have the APOE-e4 gene. A well-known fact that we all inherit a copy of each gene from each parent. Those who inherit one copy of altered APOE-e4 from their mother or father have an increased risk of developing Alzheimer’s. Those who inherit two altered copies from their mother and father (due to random assortment) have an even higher risk, but not a certainty. Besides, APOE-e4 may tend to make symptoms appear at a younger age than 65, depending on the level of mutation in the gene itself.
APP (Amyloid precursor protein (APP) discovered in 1987, is the first gene with mutations found to cause an inherited form of Alzheimer’s. This gene is directly related to amyloid formations in the brain.
Variations in PS1 and PS2 (presenilin-1,2) are also a common cause of familial AD. Early-onset familial AD, in most cases, is a result of APP, PS1, PS2 autosomal dominant mutations, which means that one copy of an altered gene from one parent is enough to trigger the disease.

In most cases, genetic risk only becomes problematic when coupled with a particularly unhealthy lifestyle and environmental factors. Nowadays, a science called epigenetics studies the correlation of genetic predisposition and environmental attributes of the disease. Such outer factors in AD can be heart disease, hypertension (high blood pressure), diabetes, heavy alcohol consumption, and even brain injury can increase the likelihood of developing AD.
Recent studies suggest that traumatic brain injury (TBI) can be a very robust factor, leading to AD or dementia advancement. Numerous in vivo studies demonstrate the following pathophysiology – Aβ plaques are reported in up to 30% of post-mortem TBI patients. There is a suggestion that TBI may induce the acceleration of misfolded protein formation and aggregation, possibly through axonal damage during brain injury, and perhaps building upon the pathogenesis of AD.
Alterations in this vascular system contribute to a reduction in global cerebral perfusion leading to brain dysfunction and cognitive impairment. Furthermore, high blood pressure promotes atherosclerosis in cerebral arteries, blocking the cerebral blood supply (Ninomiya et al., 2011), leading to lacunar or cortical infarcts, and, ultimately, cognitive impairment. It has been suggested that the link between cerebrovascular disease (CVD) and AD is even much more important than the influence of aging (Love and Miners, 2016). Some of these common risk factors shared between CVD and AD are hypertension, diabetes, atrial fibrillation, atherosclerosis, hypercholesterolemia, and apolipoprotein E (ApoE) genotype.
Cerebral amyloid angiopathy (CAA) is a condition where Aβ deposits accumulate within the walls of the meningeal and intracerebral arteries, arterioles, and very rarely, veins and capillaries. It engenders a thickening of vessel walls and constriction of the vascular lumen, thereby promoting potential micro-aneurysms. This pathology increases the risk of developing hemorrhages, ischemic lesions, and encephalopathies, resulting in profound cerebral damage that contributes to neurodegeneration and cognitive dysfunction (Ellis et al., 1996; Haglund et al., 2006). CAA is associated with a more rapid cognitive decline in demented and non-demented persons (Pfeifer et al., 2002). Certainly, CAA has a close association with AD and additive effects on the risk of developing dementia through AD pathology.
Heart disease (atrial fibrillation, arrhythmias, or cardiac arrest) causes a reduction in cerebral perfusion, leading to nerve cell damage (Kwok et al., 2011), brain dysfunction, and cognitive decline (Alosco et al., 2013).

Sleep-wake cycle disturbances are proposed as one of the earliest symptoms seen in AD. A usual sleep cycle consists of several stages N1, N2, N3( non-rapid eye movement (NREM) sleep), followed by REM sleep. During REM sleep, the brain is highly active as it is being rewired and is considered the most critical part of the sleep-wake cycle. With aging, the sleep pattern is altered by a reduction in sleeping time and REM sleep.
An increase in the amount of light throughout the sleep-wake cycle leads to an increase in insoluble tau and memory impairment since continuous light input suppresses the production of the hormone melatonin that regulates the sleep-wake cycle (Di Meco et al., 2014)
A MeDi consists of a low intake of saturated fatty acids, such as meat and poultry; a low-to-moderate consumption of dairy products, such as cheese and yogurt; a moderate amount of alcohol, such as wine; and a high intake of vegetables, legumes, fruits, cereals, fish and unsaturated fatty acids.
Medi has been shown to reduce oxidative stress by decreasing intracellular reactive oxidative species, apoptosis, and cells containing telomere shortening.
Several studies point out that the polyphenols in the natural olive oil in the MeDi regimen are the main active components to prevent AD (Omar et al., 2018). Oleuropein aglycone, present in extra virgin olive oil, induces autophagy, decreases the amount of aggregated proteins, reduces inflammation, and improves cognitive function seen in AD (Grossi et al., 2013; Cordero et al., 2018).
On the contrary, a high-fat diet (HFD) raises the risk of developing obesity, leading to increased chances of developing diabetes and, therefore, promoting the development of cognitive deficits, and perhaps AD.
This disease is characterized by feelings of sadness and loss of interest in ordinary things. A common triad of symptoms seen includes anhedonia, low energy or fatigue, and depressed mood. Depression is a common symptom seen in people suffering from AD (Drevets and Rubin, 1989; Lyketsos et al., 1996). There is a debate about whether depression is a risk factor for developing AD, rather than just a symptom. Recently, several clinical studies bolstered the idea of depressive symptoms as a crucial risk factor for cognitive decline and AD.
Neurotransmitters like dopamine and serotonin play a crucial role in the development of depression and AD pathology (Chen et al., 1996; Jacobsen et al., 2012). Serotonin helps regulate mood, social behavior, and memory, whereas dopamine functions in motor control and reward-motivated response. Therefore, these two neurotransmitters could be vital in the conversion of depression into AD. In AD mice, dopaminergic neuronal loss in the midbrain leads to memory impairment (Nobili et al., 2017), whereas restoration of dopamine release improves cognitive dysfunction (Guzman-Ramos et al., 2012). In depression, there is a decrease in dopamine production, leading to a loss of reward-motivated and low levels of serotonin have been associated with depressive behavior since serotonin regulates mood and social behavior.
Stress increases the production of Aβ and enhances the formation of amyloid plaques by increasing corticotropin-releasing factor release, which leads to an increase in neuronal activity, stimulating the production of Aβ, and demonstrating a link between depression and AD development (Dong and Csernansky, 2009).
Smoking leads to cognitive impairment and decline shown by faster reductions in verbal memory and slower visual search speeds (Richards et al., 2003). Additionally, cognitive decline in smokers is directly proportional to the number of packs they smoke per day (Kalmijn et al., 2002). Indeed, it is known that smoking has adverse effects on cardiovascular diseases, which, as mentioned, are risk factors of AD, stressing out the deleterious importance of tobacco in promoting dementia. Historically, smoking has been considered a preventative measure from developing AD, as many have stated that nicotine improves short-term cognitive performances and inhibits amyloid formation (Brenner et al., 1993; Lee, 1994). Nicotine has been proven to reduce APP secretion (Lahiri et al., 2002), inhibiting Aβ aggregation. The mechanism by which smoking may lead to an increased risk in AD development is uncertain. Further studies need to be conducted for potential mechanisms responsible for a possible increased risk of AD development.

Alcohol consumption is considered a significant risk factor for many health problems. A combination of smoking and drinking can have a more impactful effect on AD incidence than just one of those habits (Zhou et al., 2014). A potential mechanism proposed for alcohol to induce AD is by decreasing lymphatic function (Lundgaard et al., 2018). The lymphatic system plays an integral part in removing brain waste, including Aβ.
Since alcohol decreases glymphatic function, heavy drinking could induce Aβ accumulation by reducing its clearance triggering the cognitive abnormalities seen in alcohol use and AD.
- Lack of physical activity
Under normal circumstances, an elderly individual without dementia diagnosis will exhibit hippocampal volume shrinkage of 1%–2% each year (Erickson et al., 2011).
AD patients performing a moderate exercise program for a year exhibited a slower decline in the capability to achieve daily living activities and amelioration of the physical impairment (Rolland et al., 2007; Pitkälä et al., 2013). Some other studies have also found that aerobic exercise can improve memory performance and cognitive function in aging. Although all these studies indicate that exercise may be useful in reducing the clinical symptoms observed in AD patients, no reviews report its effect on amyloid deposition and how physical activity may prevent developing AD in the at-risk population.
Most of the studies compiled in this review evaluate the effect of risk factors when the AD-associated pathological changes are already present. Still, very few analyze the potential factors in preventing the onset of the disease, rather than further development. Hence intervention of potential risks is highly recommended for either prevention or even amelioration of clinical symptoms of AD since most of these actions will also benefit general health status.

Finding therapy for Alzheimer’s disease (AD) is perhaps the greatest challenge for modern medicine. So far, there are not many current treatment methods, and there is no specific targeted drug. For blocking the disease progression, medications have to interfere with all pathogenic steps, which are responsible for all the clinical symptoms- formation of amyloid plaques, neurofibrillary tangle formation, inflammation, and oxidative damage, and metabolism dysregulation.
However, modern medicine suggests the following:
Cholinesterase inhibitors (CIs)
A proposed strategy is to help CIs enhance cholinergic transmission to delay the degradation of acetylcholine between the synaptic cleft. For now, there are three CIs approved for the treatment of mild to moderate AD:
- Donepezil (Pfizer, New York, NY, USA);
- Rivastigmine (Novartis, Basel, Switzerland);
- Galantamine (Janssen, Beerse, Belgium) (Farlow et al., 2002).
The following drugs have been regarded as the standard and first-line treatment for AD.
N-methyl- D-aspartate antagonist
Another therapeutic option for AD moderation is called memantine (Lundbeck, Valby, Denmark). This drug serves as an uncompetitive and moderate-affinity N-methyl-D-aspartate (NMDA) antagonist. It is believed to play a neuron-protective role from excitotoxicity. However, there are frequently reported adverse events in memantine trials- dizziness, headache, and confusion.
Combination therapy
Studies by Tariot. et al., 2004 showed that from combination use of memantine and donezepil showed a significant benefit in parallel groups of patients with moderate to severe AD symptoms over placebo groups of patients. Such therapy showed a gradual increase in cognitive function, language, ADL, behaviors, and the global state of patients.
Treatment of psychological and behavioral symptoms
According to a large observational study, behavioral symptoms can be divided into four major groups with high prevalence: 38 % psychosis (e.g., delusions), 59% affective symptoms ( anxiety, depression), 64% hyperactivity (reactivity, aggression, disinhibition) and 65% apathy. (Zec and Burkett, 2008).
- Psychotic symptoms and agitation/aggression in AD patients are commonly treated with antipsychotics (olanzapine, risperidone, quetiapine, ziprasidone, and aripiprazole).
- For depression episodes, combined selective noradrenaline and serotonin inhibitors (SNRIs), such as Mirtazapine, venlafaxine, and duloxetine, are widely used as antidepressants.
- The class of benzodiazepine drugs is used to reduce agitation and anxiety.
Despite decent efficacy levels and widespread use, all of these medications have serious adverse effects. For instance, acetylcholinesterase inhibitors may cause diarrhea, nausea, vomiting and significant weight loss (Kaduszkiewicz et al., 2005), while memantine is sadly known to cause hallucinations, dizziness, and fatigue (Herrmann et al., 2011)
It is evident that drugs currently used for the treatment of AD have weak beneficial effects on cognitive function or offering some relief. They slow down but do not stop or reverse the disease progression, highlighting the need for new, more effective therapeutics.

CBD (also known as cannabidiol) is a naturally occurring compound found in the cannabis plant. In fact, CBD is one of over 100 compounds originated from the cannabis plant, including THC (delta-9 tetrahydrocannabinol), terpenes, flavonoids, omega fatty acids, and others.
It’s fair to ask how this substance affects well-being. It is a typical false impression that CBD has the same psychedelic effect as THC. However, CBD is entirely non-psychoactive, which means it does not create the euphoric feelings associated with other types of cannabis compounds. CBD, extracted from industrial hemp, contains less than 0.3% THC, which is considered legal.
People who currently use CBD products claim that CBD helps them to feel calm and relaxed and thus even helps them cope with everyday life problems. Depending on the type of cannabis strain and proportion of compounds in it (for instance, CBD: THC ratio), there is a considerable variety of other beneficial effects. Cannabidiol is available on the market in different forms, such as tinctures, edibles, oils, liquids for vaping, flower buds from smoking joints, etc. So anyone can choose a suitable way of consumption up to their preferences.
In 2006 a team of University of Connecticut researchers published a study in Molecular Pharmaceutics reporting that cannabis “could be a considerably better suppressor of the malformed proteins abnormal clumping than any currently prescribed treatments.” We can only hope that predicted cannabinoid-based medications “will be the new breakout medicine treatments of the near future.”
Some studies suggest cannabis could help to manage:
- Behavioral symptoms of dementia (agitation and aggression)
- Nausea relief
- Good sleep promotion/ help with insomnia
- Pain ease
- Anxiety, depression reduction
- Improvement of cognitive abilities and memory
- Cancer-related symptoms alleviation
- Acne treatment
- Antioxidant (reduce oxidative stress)
- Diabetes prevention
- Substance abuse treatment
- Antipsychotic effect
Minor side effects of cannabis consumption
- Mouth dryness
- Lowering of blood pressure
- Drowsiness
- Fatigue
- Can interfere with other medications
The science behind CBD
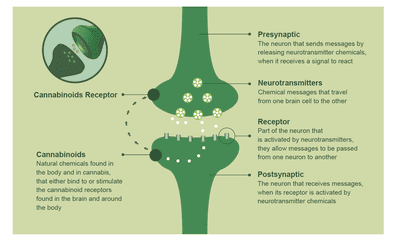
In 1990 it was discovered that there are endocannabinoids (“endo “means “originating within the body”), which are the constituents of the endocannabinoid system in the human organism. They act as a bioregulatory mechanism for most inner processes and have receptor sites throughout the body. So, the two key eCBs circulating in your body are Anandamide and 2-ArachidonoylGlycerol.
The Anandamide molecule operates throughout the endocannabinoid system and is involved with appetite, memory, and even pregnancy. 2-AG has been associated with our emotional states, protection from seizures, and maintaining cardiovascular health. Even more, 2-AG is responsible for the feeling of orgasm during sexual intercourse.
Cannabinoid receptors (CB1 and CB2)
CB1 receptors are among the most spread receptors in the entire nervous system, which makes them essential for the healthy functioning of the brain. Depending on what area of the brain they are located in, they can be regulators of your mood, memory, motor function, or perception of pain. However, when THC binds to CB1 receptors, it can activate the psychoactive properties of cannabis.
The highest density of CB2 receptors is found in the immune system, especially in the spleen. These CB2 receptors are responsible for the inflammation moderation and our immune response to pathogens. In terms of therapeutic effects, CBD plays a more vital role than CB1, which we will discuss further.
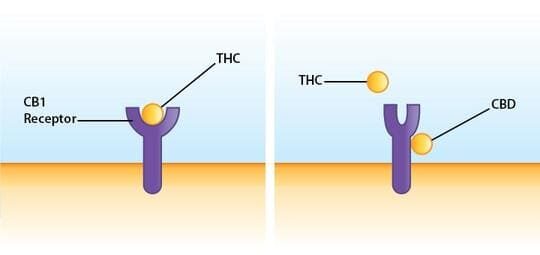
Most cannabis compounds can bind to both CB1 and CB2 types of receptors, and this is also true for both the endocannabinoids — Anandamide & 2-AG. However, the phytocannabinoid CBD doesn’t directly trigger either receptor. Instead, it modifies the receptors’ ability to bind to cannabinoids.
The ECS regulates most physiological systems in the body, but above all, the nervous system helps achieve the balance that allows individual nerve cells to communicate. The ECS is disrupted in both Alzheimer’s and Parkinson’s diseases.
How CBD works
- First, CBD weakly activates cannabinoid type II (CB2) receptors, which reduce the inflammatory response.
- Secondly, CBD blocks the breakdown of the brain’s endogenous cannabinoid, 2-AG, by modifying the receptor and thereby increasing 2-AG levels and further activation of CB2 receptors.
- Lastly, CBD activates the PPARg receptor, which reduces brain inflammation in AD.
Both PPARg receptor activators and microglia inhibitors have shown promise in human clinical trials but have been limited by prohibitive side effects. CBD may achieve these effects with a better side effect profile.
In a mouse model of PD, treatment with nabiximols (Sativex®), cannabis-based pharmaceutical approved in 30 countries outside the USA, resulted in improvement in dopamine neurotransmitter function, and reduced oxidative stress (akin to “rust” of the nervous system), as well as leading to improvements in anxiety and self-injury behaviors.
Both THC and particularly CBD are known to be neuroprotective agents that hold the potential to slow or perhaps even halt the degenerative process. On the symptom side, THC as a single agent has proven beneficial in AD patients in reducing nocturnal agitation, improving sleep, and appetite. There is also the possibility of making a real difference in slowing or abrogating the pathological processes in Alzheimer’s, but so far, there are only rodent trials available.
A study by Ana M.Moreno et al., 2011 has investigated the effects of CBD on cognition in a pharmacological model of AD. Three-month-old mice were intraventricularly injected with 2.5 μg of fibrillar Aβ. Then they were treated with 20 mg/kg CBD using daily injections for one week and later three times/week for the following two weeks. To observe the CBD treatment effect, mice were assessed in spatial learning (Morris Water Maze), the social preference test, and fear conditioning paradigms. (A. Moreno et al., 2011. )This study was the first to demonstrate CBD’s ability to prevent social recognition deficits (which is a common hallmark of AD). Treatment was able to reverse the cognitive deficits of Aβ-treated mice. Hence, it provides the first evidence that CBD may potentially be a preventative treatment for AD, particularly relevant for social withdrawal symptoms and facial recognition.
The combination of CBD and THC also showed efficacy in AD-related processes in vivo. One of the studies conducted by Casarejos et al. (2013) investigated Sativex’s effects in a mouse model with tauopathy. This mouse model was primarily a model for frontotemporal dementia, parkinsonism, and lower motor neuron disease. Sativex treatment was shown to decrease gliosis, increase the ratio of glutathione, which is a body antioxidant, thereby showing neuroprotective and antioxidant properties. Importantly, Sativex showed a reduction of Aβ and tau deposition in the hippocampus and cerebral cortex and increased autophagy (Casarejos et al., 2013), thus implying that although the mouse model is not directly related to AD, the therapeutic benefits are.
In 2015 the second study conducted by Aso et al. compared the effect of CBD, THC, and a CBD-THC combination in the APPxPS1 (mutated APP and PS1 genes) mice. Even though mice had an early symptomatic phase of AD (~6 months), all types of treatment improved memory deficits in the two-object recognition task. Interestingly, only CBD-THC combination could prevent the learning deficit seen in the active avoidance task. It also decreased soluble Aβ42 levels and changed plaque composition while CBD and THC individually did not (Aso et al., 2015).
Antioxidant
Oxidative stress, as mentioned earlier, is another key contributor to Alzheimer’s disease progression. It further leads to the production of reactive oxygen species (ROS) or so-called free radicals that interfere on the cellular level. ROS play an essential role in several cellular and signaling pathways at physiological concentrations (cell cycle regulation, phagocytosis, and enzyme activation), hence, excessive generation of ROS leads to several harmful effects including DNA, lipid, and protein damage. Additionally, when Amyloid Beta-protein is present, it elevates a reactive type of oxygen species even more in the adjoining cells through the membranes’ exchange process.
The overall oxidative stress process leads to neuronal loss along with the deprivation of synapses within the brain, which therefore leads to memory loss and other neurological symptoms. You may ask how cannabis can help?
THC and CBD are potent antioxidants with anti-inflammatory properties. As brain inflammation is thought to be a significant contributor to AD, there is no surprise that anti-inflammatory drugs, like non-steroidal anti-inflammatory drugs (NSAIDs; e.g., ibuprofen) reduce the risk for developing AD. But if these drugs are used chronically, they can interfere with kidneys and liver work. It was already shown and tested that CBD can be widely used with limited side effects, and are mostly considered safe for adult and senior use.
Microglia inactivation
Microglia are brain cells, similar to neurons. They comprise 10% of the brain cells and are activated following injury or disease, like an immune response of the brain. Although the purpose of microglia is to protect other brain cells, their chronic activation leads to more harm than good. Activated microglia release glutamate, cytokines, and other harmful substances which, over time, kill neurons. So, CBD helps to reduce microglia activation through CB2 receptors interaction. Not surprisingly, activated microglia is another less commonly known hallmark of AD pathogenesis. When other medications stop microglia from producing harmful substances but also showing side effects, CBD offers a well-tolerated strategy.
Neuron protection
Meanwhile, it’s useful to say that since 2003, the US federal government has held a “medical patent” for the marketing of cannabinoids as neuroprotective agents. The patent states that cannabinoids are “useful in the treatment and prevention of a wide variety of associated oxidation diseases such as inflammatory and autoimmune diseases. The cannabinoids are found to have particular applications in limiting neurological damage following ischemic insults, such as stroke and trauma, or in the treatment of neurodegenerative diseases like Alzheimer’s disease, Parkinson’s disease, and HIV dementia.”
CBD has shown a great result in alleviating AD symptomatology and promising conclusions in preventing AD disorder in rodents. However, due to ethical reasons, there are still no studies on people to determine the effects of CBD oil or its components on the treatment of AD.
According to Redstorm Scientific here is the list of the top 10 cannabis strains which help in treating Alzheimer’s disease:
- Electric Kool-Aid (Hybrid)
- Dutch Dragon (Sativa)
- Acapulco Gold (Sativa)
- Lavender Haze (Sativa)
- Green Crack (Sativa)
- Bio Jesus (Hybrid)
- LSD (Hybrid)
- White Russian (Hybrid)
- The OX (Indica)
- Blissful Wizard (Hybrid)
Most commonly prescribed CBD oils for AD patients:
- CBD Pure (CBD isolate)
- Elixinol
- Koi CBD
All of these oils are strictly THC free, organic, and derived from industrial hemp.
Correct dosage of CBD
We already understood that any inflammation is a signal that your body’s homeostasis is not maintained. However, everyone’s endocannabinoid system, responsible for homeostasis regulation, is unique and finding a standard dose for any ailments. Lauren Wilson, the co-author of the book “Healing with CBD,” suggests that potential consumers should first consult their doctor and do the research before stepping onto CBD track because CBD can interact with other prescribed drugs making them more or less effective. Also, anyone can start to keep track of the CBD treatment journal to observe how the CBD makes you feel. You can write down a dosage they’re taking, which product, and how it makes you feel, find your optimal dose, or in scientific terms, a “sweet spot.” But it is essential to understand that the sweet spot will be different for everyone.

Dr. Ethan Russo, a board-certified neurologist and a current director of Research and Development of the International Cannabis and Cannabinoids Institute, strongly recommends not to wait when the first signs of dementia appear, but to tackle them in advance. Here are some of the preventative activities you should do to lower the risk of AD:
- The best current approaches beyond the current pharmacopeia offers include an active lifestyle: aerobic activity and daily mental exercises.
- Mediterranean diets (rich in monounsaturated olive oil and omega-3 fats from fish) with anti-inflammatory fruits and berries are strongly recommended.
- Use of probiotics and prebiotics. You can easily find such cultivated medium in shop organic multi-culture yogurts, kefir, Lacto-fermented vegetables, and supplements in capsules. Prebiotics from vegetable matter like acacia fiber, slippery elm, burdock root, and again supplement in pills) provides an optimum feedstock for the beneficial gut bacteria.
- Use of potential antioxidants like mitoquinone, vitamin E, Ginkgo biloba, natural polyphenols such as green tea, wine, blueberries and curcumin, fatty acids, folic acid, vitamin B6, and vitamin B12 supplementations.
- Regular physical activity (which is healthy in many cases).
- Lowering the risk of stress, but we all know that, unfortunately, it is inevitable. CBD provides an excellent remedy for preventing anxiety and reducing your inner worries
- Quit unhealthy habits such as smoking and alcohol abuse.
- An alternative solution to dosing with phytocannabinoids (CBD, THC) is to boost your body’s natural endocannabinoid production. In such a way, your body can deliver eCBs to your body parts that are in the most need.

Anastasiia Myronenko
Anastasiia Myronenko is a Medical Physicist actively practicing in one of the leading cancer centers in Kyiv, Ukraine. She received her master’s degree in Medical Physics at Karazin Kharkiv National University and completed Biological Physics internship at GSI Helmholtz Centre for Heavy Ion Research, Germany. Anastasiia Myronenko specializes in radiation therapy and is a fellow of Ukrainian Association of Medical Physicists.